| Tracks 1-14 |
| Track 1 |
Introduction |
| Track 2 |
XELOX-1/NO16966: CAPOX or FOLFOX4 with or without bevacizumab as first-line therapy |
| Track 3 |
Comparable efficacy and tolerability of CAPOX and FOLFOX |
| Track 4 |
Geographic variation in the tolerability of fluoropyrimidines |
| Track 5 |
Potential impact of discontinuing bevacizumab and chemotherapy concomitantly before progression |
| Track 6 |
Continuation of bevacizumab with a fluoropyrimidine after discontinuation of oxaliplatin off protocol |
| Track 7 |
Role of xaliproden as a neuroprotectant during oxaliplatin administration |
| Track 8 |
Efficacy of xaliproden in the prevention of and recovery from neuropathy |
|
| Track 9 |
AVANT adjuvant trial: FOLFOX with or without bevacizumab or CAPOX with bevacizumab |
| Track 10 |
Bevacizumab and long-term safety |
| Track 11 |
Potential advantages of panitumumab, a fully humanized monoclonal antibody against EGFR |
| Track 12 |
Incorporation of combination biologic therapies in adjuvant clinical trials |
| Track 13 |
Oral small-molecule pan-VEGFR tyrosine kinase inhibitor AZ2171 |
| Track 14 |
Novel agents in development for colorectal cancer |
|
|
Select Excerpts from the Interview
Track 3
 DR LOVE:
DR LOVE: Can you review the data you presented at the ASCO GI
Cancers Symposium on the XELOX-1/NO16966 trial?
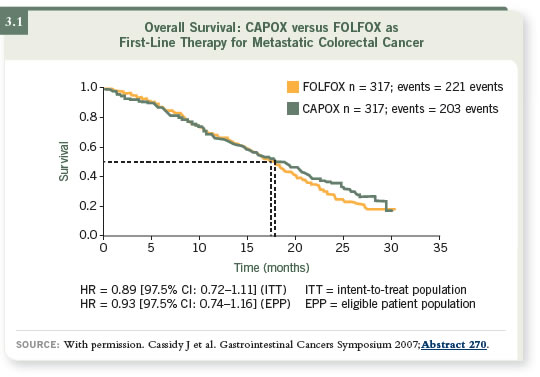
DR CASSIDY: The initial randomization was to CAPOX versus FOLFOX.
There’s absolutely no chance statistically that CAPOX has any inferiority, and
we’re even more confident now that we have overall survival statistics to back
that up (Cassidy 2007; [3.1]). We’re confident that CAPOX is noninferior
to FOLFOX. The lines cross each other depending on the populations used
— the intent-to-treat or the eligible patient populations.
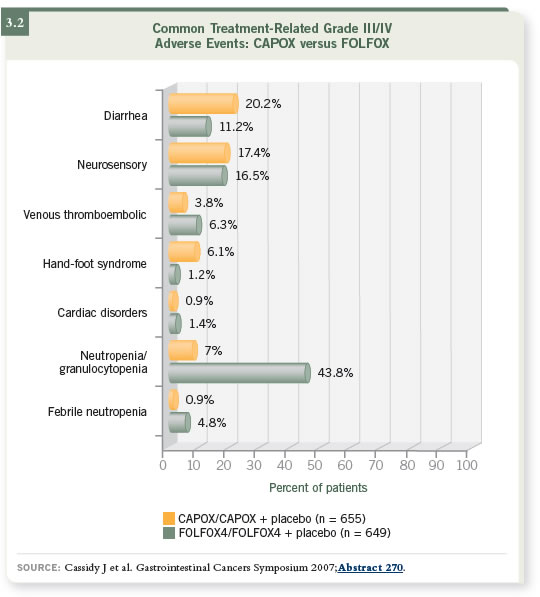
One consideration in trying to pick a winner between these regimens is the
side-effect profile of the regimen (3.2). In my mind, that discussion has no
clear winner.
What swings it for me is what we started off with, which was the hypothesis
that CAPOX would be a simpler treatment for patients and would be easier to
deliver. That’s what makes CAPOX the better regimen.
Track 5
DR LOVE: Can you discuss the bevacizumab results from the trial?
DR CASSIDY: A progression-free survival advantage was evident with the
addition of bevacizumab to both chemotherapy regimens (Cassidy 2006a).
One issue that caused some people concern is that the quantum of benefit with
the bevacizumab- and oxaliplatin-containing regimens is less than what was
seen with IFL and bevacizumab in the original Hurwitz data. The absolute
difference in median progression-free survival associated with bevacizumab in
the Hurwitz data was about four months (Hurwitz 2004), and in our study it’s
about one and a half months (Saltz 2007). We’ve been thoroughly examining
why that might be.
The best hypothesis we have at the moment is that although the protocol
allowed patients to stop oxaliplatin or the fluoropyrimidine and continue
bevacizumab, the majority of patients discontinued bevacizumab when the
chemotherapy stopped. That occurred at around six months for a large proportion
of the patients in the trial (Saltz 2007). In contrast, most of the patients in
the Hurwitz trial continued bevacizumab for a longer time — until progression.
DR LOVE: How do you approach these cases in a clinical setting with regard
to that issue?
DR CASSIDY: We would continue patients on therapy until progression. When
patients develop oxaliplatin neuropathy, then we reduce the dose of oxaliplatin
or we discontinue the oxaliplatin. We would continue with the fluoropyrimidine
and bevacizumab.
Track 7
DR LOVE: Can you discuss your work with xaliproden?
DR CASSIDY: Xaliproden is a potential neuroprotector. It was initially tested
in patients with amyotrophic lateral sclerosis, but it didn’t work well. It’s also
been tested in patients with Alzheimer’s disease, and the results with those
patients are not yet known.
I previously presented data evaluating xaliproden as a potential neuroprotector
for oxaliplatin-associated neuropathy (Cassidy 2006b). The second
trial is essentially a confirmatory trial, but we are also trying to address some
questions that arose from the first trial.
In the preclinical models of oxaliplatin- and platinum-associated neuropathy,
the drug was active. That’s what set the ball rolling in terms of trying to
conduct clinical trials. If you have something that prevents the neuropathy
associated with oxaliplatin, then you can do two things.
First, you can administer more oxaliplatin, which might mean more activity.
Second, you can administer the same amount of oxaliplatin and avoid the
neurotoxicity. I believe both of those options are sensible and reasonable. We
chose to deliver the same amount of oxaliplatin and reduce the neuropathy,
not to administer more oxaliplatin.
DR LOVE: What do we know about the ability of xaliproden to prevent oxaliplatin-associated neuropathy?
DR CASSIDY: The first trial demonstrated a reduction in Grade III neuropathy
and an increase in Grade II neuropathy. It appeared as if you shifted patients
into a lower grade of neuropathy (Cassidy 2006b). The controversial aspect of
that trial was that we didn’t consider the duration of neuropathy after stopping
chemotherapy. For example, could you shorten the recovery period from
neuropathy? We need to consider that in the second trial.
We also demonstrated that no decrease occurred in the activity of the chemotherapy
(Cassidy 2006b). Oncologists worry about an agent being used to
prevent toxicity affecting activity. In the first trial, we definitely convinced
ourselves that was not the case. Xaliproden is an unfinished story, and the next
trial should provide a definitive answer to the question about neuropathy. It’s a
bigger trial being conducted with more detailed neurophysiology.
Track 13
DR LOVE: Can you discuss the new anti-VEGF agent, AZD2171?
DR CASSIDY: AZD2171 blocks all three VEGF receptors. It’s a bit different
from bevacizumab in that it doesn’t sequester the ligand, but it blocks the
receptors. Theoretically, that has advantages, and in preclinical models it does
appear to offer some advantages over bevacizumab.
The Horizon trials — which are planned and ongoing — are evaluating
AZD2171 with FOLFOX versus FOLFOX with bevacizumab as second-line
therapy (Horizon I), and the addition of AZD2171 to FOLFOX or CAPOX as
first-line therapy (Horizon II). Further on in the development pipeline are plans
to conduct a trial that will be a straight head-to-head comparison of FOLFOX/bevacizumab to FOLFOX/AZD2171 as first-line therapy (Horizon III).
DR LOVE: Can you talk about how it’s administered and what the side
effects are?
DR CASSIDY: The side effects are, so far, similar to what has been seen with
bevacizumab. Vague side effects like fatigue and problems with hypertension
occur — class effects you might expect. I haven’t seen anything in the toxicity
profile that makes me see it as significantly different from bevacizumab. It’s
an orally administered drug, and it’s administered daily, which is clearly an
advantage over bevacizumab for long-term administration.
Select Publications